
Viral Uncertainty
How Ambiguity and Amplification Broke Our Social Immune System

Science with the Fans on the Field
Before the pandemic, the game of science was played by experts. Journals and institutions enforced the rules, science journalists provided the play-by-play, and the public watched from the stands.
In the chaos of COVID, those boundaries collapsed. The game accelerated. The referees couldn’t keep up. Journalists struggled to be heard.
Suddenly, the fans were on the field.
And the game was life and death.
The year of fear.
Six years ago, we had just watched China lock down entire cities to contain a virus the world barely understood. Throughout Asia and in Europe, cases were rising. Deaths were mounting in Italy and spreading across the continent. The images were stark.
We braced ourselves and wondered which threat loomed larger:
The disease.
Or the measures required to contain it.
Uncertainty is the great amplifier of fear, and this virus arrived shrouded in it. Who was most at risk? How easily did it spread? How often did it kill? The realization it could occur without severe symptoms meant we didn’t even know how many cases there had been.
And everything we now know this virus explains its ability to elicit confusion. It spread before symptoms. It posed just enough risk to kill millions, but not enough to command unquestioning compliance with public health measures. And, as an RNA virus, it was a relentlessly mutating shape-shifter, constantly defying expectations and thwarting counter-measures.
At first, fear of the unknown united us. When the first U.S. death was announced on February 29, 2020, public health measures accelerated with relatively little opposition. Travel slowed. Schools closed. Businesses shuttered. The mortality curve rose sharply — and then began to bend.
But shutting down large sectors of society carried enormous economic and social consequences. Outside overwhelmed hospitals, the threat did not look the same everywhere. Different regions were experiencing entirely different pandemics. In many rural communities, cases were sparse in the early weeks. Restrictions felt abstract. In urban centers, the danger was immediate and visible.
Age compounded the divide. For older Americans, the virus posed an existential threat. For many younger adults, the risk appeared remote while the costs of intervention were immediate.
To the young — and to communities not yet touched by rising mortality — the response sometimes felt worse than the disease.
How deadly was this virus, really?
In the absence of clear answers, interpretation rushed in.
The Window of Ambiguity
Over the course of March 2020, as cases accelerated and hospitals began to fill, public health officials warned of catastrophic mortality. Interventions escalated. So did skepticism.
On March 24, two Stanford faculty members asked in a Wall Street Journal op-ed:
“Is the Coronavirus as Deadly as They Say?”

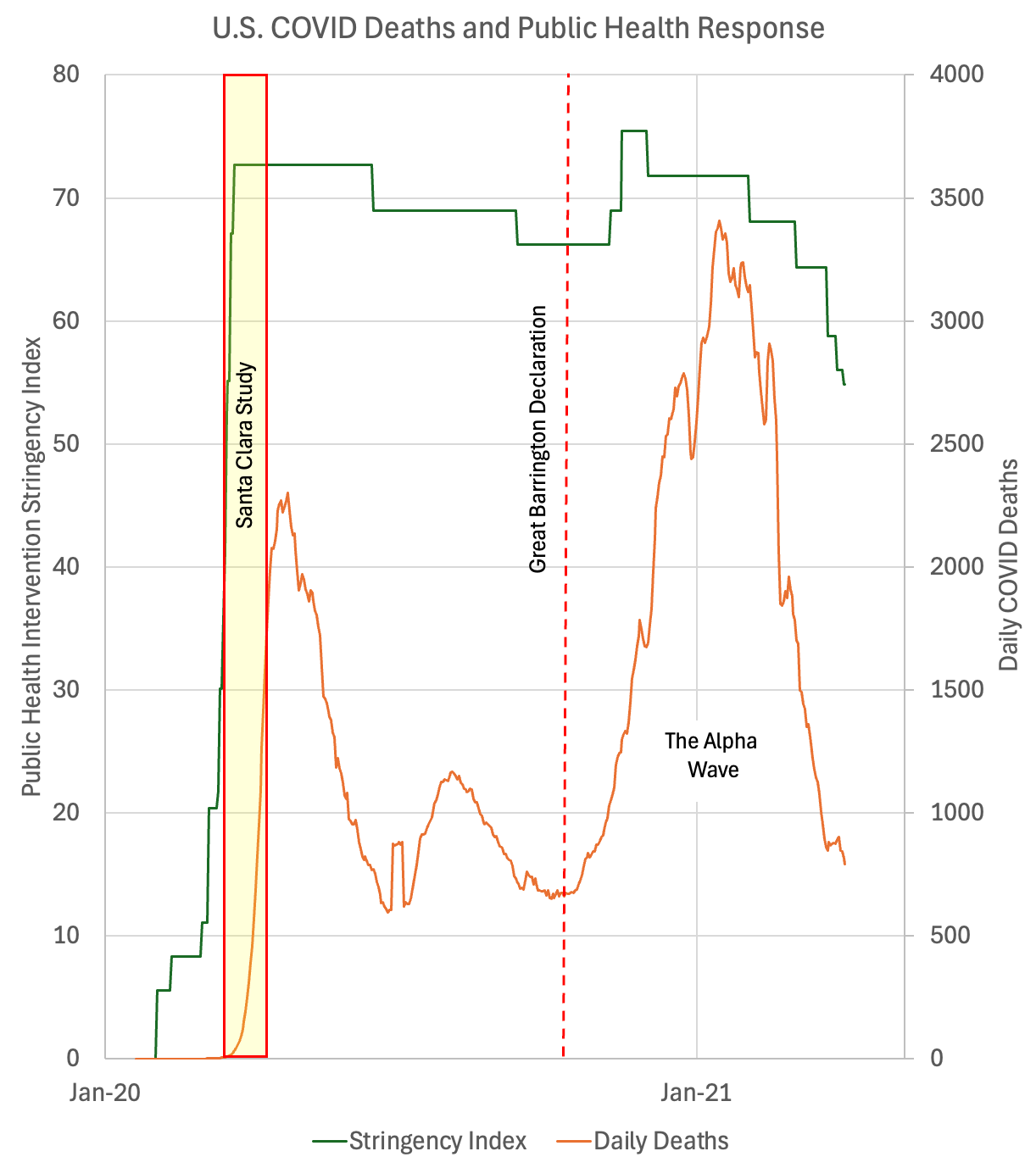
Earlier that month, the World Health Organization reported that, globally, 3.4% of confirmed cases had died. Within two weeks, its authors had launched a study to test for COVID antibodies in Santa Clara County. But they had recruited on Facebook, a procedure the WHO explicitly recommends against because of the high risk of bias in the sample. (For a detailed critique, see my post on the study.)
Within a month, the authors of the study raised funds, collected data, and put out the answer. The study concluded that the true infection fatality rate was 0.17%, a tiny fraction of the WHO estimate and only slightly higher than the flu at 0.1%.
Epidemiologists and immunologists quickly responded with critiques, but nuanced scientific discussion struggled to compete on platforms where non-experts and experts occupied the same space and algorithms rewarded outrage over calibration. No one wanted the public health measures. This seemed to offer a reason to ignore them.
A large and growing swath of the population became convinced, regardless of expert opinion, that the risk of COVID was overblown—that it was actually no worse than the flu.
The Amplifier
The Santa Clara preprint did not simply enter the scientific record. It entered the algorithm.
Preprints were not new in 2020, but their role in medicine was. MedRxiv had launched only months before the pandemic. For the first time, clinical and epidemiologic claims could circulate globally before peer review.
This shift was not inherently problematic. In a fast-moving pandemic, rapid dissemination was essential. Traditional medical publishing — often requiring nine months or more from submission to print — was structurally incapable of keeping pace with exponential spread.
Journals dropped paywalls. They fast-tracked COVID manuscripts. Retractions increased. The system strained to accelerate without abandoning standards.
Preprints filled the speed gap.
But preprints were never designed for mass public consumption. They were tools for expert communities. In 2020, the fans left stands and the game would never be the same.
Twitter had already become a primary platform for scientific exchange. During COVID, it became a public battleground. Claims released on preprint servers were debated in real time by epidemiologists, political commentators, and journalists. But influencers, onlookers, and trolls flooded the zone. Algorithms rewarded engagement, not calibration.
The Santa Clara estimate — released as a preprint — was ideally suited for this environment. It was simple. It was reassuring. It appeared to contradict dire projections.
And it traveled faster than critique.
By the time the paper underwent peer review more than a year later, the debate it had ignited had already reshaped public discourse.
This was not merely a flawed study amplified by social media.
It was an information ecosystem in which speed outpaced verification, and confident narrative framing could precede evidentiary consolidation.
That architecture mattered.
From Santa Clara to Great Barrington
The lead author of the Santa Clara study would later co-author the Great Barrington Declaration in October 2020, which argued for “focused protection” — shielding the elderly while the virus ran its course in the broader population as they returned to “normal”. What began as an estimate of infection fatality rate evolved into a coherent alternative public health philosophy.
There is no way to calculate the impact of this philosophy with certainty, but over the next four months Alpha variant would kill a quarter of a million Americans in the deadliest wave of the entire pandemic. As it did, the stringency of public health measures rose, but only briefly. Then, before it was over, they plunged.
The influence COVID minimization gained during the ambiguity window did not dissipate when evidence accumulated. It persisted. Two competing pandemic narratives emerged. In one, it posed a grave threat—one we should all work collaboratively to minimize. In the other, it was an overblown threat, foisted on us by an over protective public health community that did not respect individual freedoms.
Estimates released in uncertainty shaped risk perception. Risk perception shaped policy debates. Policy debates shaped action — and inaction. In a pandemic, timing matters. Delays matter. Narratives matter.
The social immune system did not fail in a single moment.
It broke in two.
A terrific piece - but an important note to add concerning the Great Barrington Declaration is that it was NOT a spontaneous expression of legitimate scientific opinion but a heavily subsidized, deliberate effort by fossil fuel interests (particularly the Koch brothers) to minimize concern about COVID for both financial and ideological reasons. Whether they hand picked bad scientists before or after those scientists came to their erroneous conclusions is less clear but maybe not so important.
Thank you for featuring the dreadful Clara County pseudo-research, which should have destroyed John Ioannidis's reputation forever. And in any case, as a researcher with >70 articles as first author I think his famous "Why Most Published Research Findings Are False" is a lousy paper, based on trivial and/or obvious statements.